
Rituximab
Amanda Days
Biomedical Sciences
Introduction to Immunology BIOL 302
Professor Clayton Wright
1/27/2023
Monoclonal antibodies are a commonly used component in the diagnosis and treatment of many different pathogens and diseases (3). They can range from a variety of shapes and sizes, the basic structure being a “Y” shape (3). The purpose of this technology was to improve immunotherapy and to encourage the immune system to target cancer cells on its own (1). The development of these types of antibodies (mAbs) as a use for potentially therapies began in 1975, and by 1988, rituximab was developed. The development of this specific drug came from the use of monoclonal antibodies to identify B-cell restricted antigens like CD19 and CD20 (5). From this, it was known that mAbs could then be used on tumors that expressed those specific antigens by treating the tumor with an anti-CD20 mAb (5). This eventually led to rituximab’s creation, or the creation of a chimeric anti-CD20 mAb that has increased antitumor activity and contains IgG1 regions (5). The Food and Drug Administration granted the intravenously administered version of rituximab approval in 1997, and was the first mAb to be used for oncological practices (5). The effectiveness of this drug comes from its affinity for the B-lymphocyte transmembrane protein, CD20, which can be found on normal cells and on most of the malignant cells (5). The overall mechanism begins with the drug binding to CD20 on the surface of the B-cell which in turn causes a signaling cascade that generates the membrane attack complex which eventually leads to phagocytosis (5). The dosage for this drug is 375 mg/m2, given monthly, and some serious side effects include vision problems, infections, skin sores, chest pain, dizziness, etc. depending on the patient’s condition requiring treatment (4). Alternative names for the drug include Rituxan, Ruxience, or Truxima, and they are manufactured by Genetech. Figure one indicates the general structure of the drug (5).
While the exact mechanism of Rituximab is unknown, it is understood that the drug is specific in binding to and has high affinity for the CD20 antigen (5). There are four different proposed mechanisms for the elimination CD20 cells being antibody-dependent cellular cytotoxicity (ADCC), complement-dependent cytotoxicity (CDC), antibody-dependent cytotoxicity, and lastly direct antitumor effects through apoptosis or other forms of cell death (5). After the fragment crystallizable portion of rituximab mAb binds to tumor cells, CD 20 reorganizes into lipid rafts which causes a signaling cascade, leading to CDC, phagocytosis, and cell lysis (6). If the fragment crystallizable region of the drug binds to the membrane bound Fcy receptors on effector cells, then ADCC will occur (5). Nonclassical apoptosis occurs when rituximab binds to CD20 on B lymphocytes which causes the crosslinking of many CD20 molecules (5). The key takeaway from this information is that the drug helps the body utilize the defense mechanisms that are already in place to fight off tumor cells, cancer, etc. After Rituximab tags the target cells, they can either be destroyed or induced for cell apoptosis to stop or limit the disease causing harm to the body. This would already improve disease symptoms by removing the cause of the disease, or at the least, reduce the symptoms that were being created. One study’s results showed that Rituximab was effective in mediating various B-Cell lines which the amount of complement inhibitory molecules expressed on the malignant B-cells correlates with in vitro lysis, this particular mechanism being effective against follicular lymphoma (6). Another demonstrated its effectiveness against acute lymphoblastic leukemia by using the drug alongside chemotherapy, which seemed to improve the patient’s outcome (2). While it improved the patients’ outcome, it also helped prevent reactions to certain ingredients in the chemo (2). Overall, the studies have shown effective results in the use of rituximab and the combined use of it and other therapies seemed to have even better results.
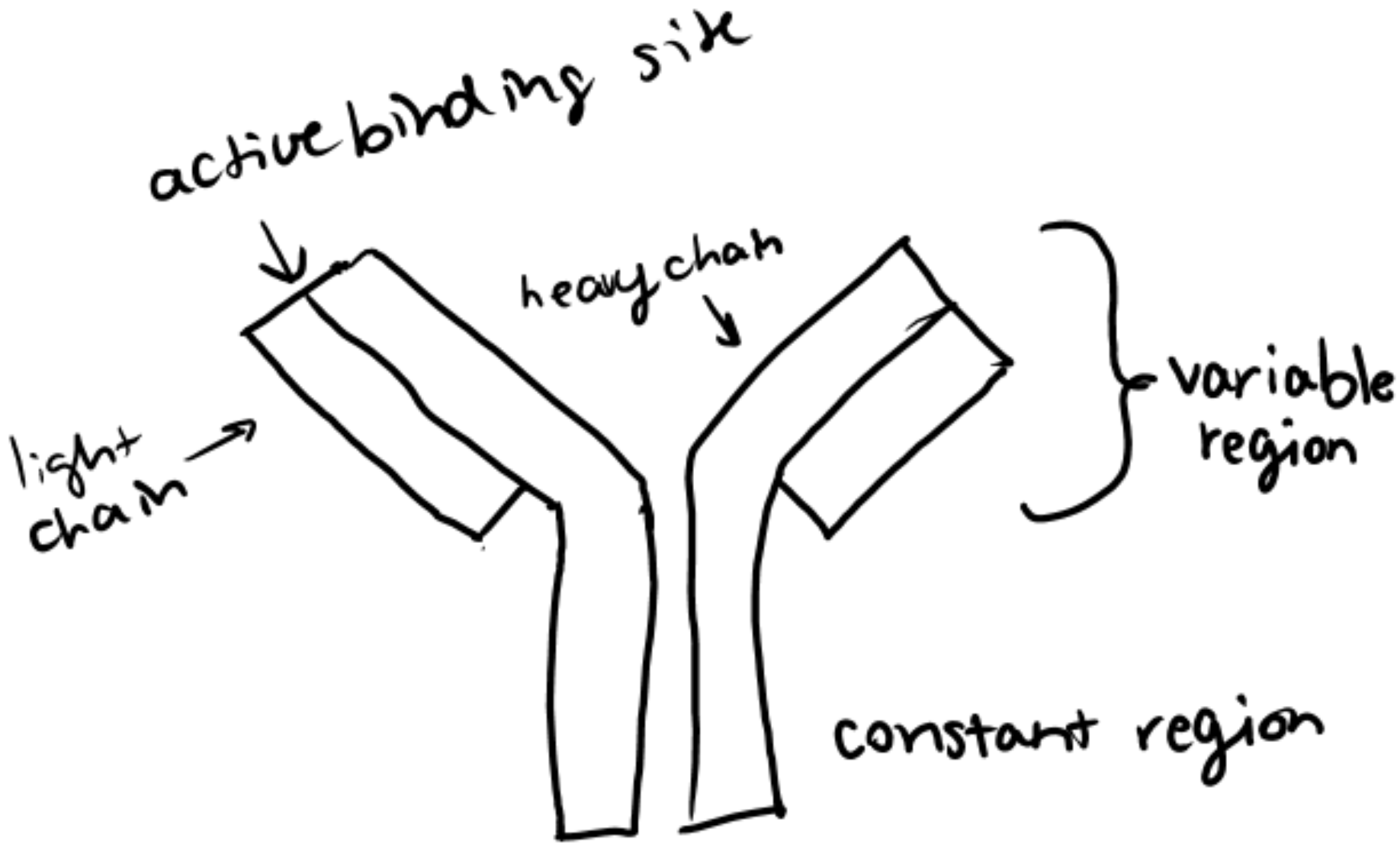
Figure 1: Sketch of the structure of Rituximab.
Sources:
1) Kimiz-Gebologlu, I., Gulce-Iz, S., & Biray-Avci, C. (2018). Monoclonal antibodies in cancer immunotherapy. Molecular Biology Reports, 45(6), 2935–2940. https://doi.org/10.1007/s11033-018-4427-x
2) Maury, S., Chevret, S., Thomas, X., Heim, D., Leguay, T., Huguet, F., Chevallier, P., Hunault, M., Boissel, N., Escoffre-Barbe, M., Hess, U., Vey, N., Pignon, J.-M., Braun, T., Marolleau, J.-P., Cahn, J.-Y., Chalandon, Y., Lhéritier, V., Beldjord, K., … Dombret, H. (2016). Rituximab in B-lineage adult acute lymphoblastic leukemia. New England Journal of Medicine, 375(11), 1044–1053. https://doi.org/10.1056/nejmoa1605085
3) Nelson, P. N. (2000). Monoclonal antibodies. Molecular Pathology, 53(3), 111–117. https://doi.org/10.1136/mp.53.3.111
4) Rituximab uses, dosage, side effects & warnings. Drugs.com. (n.d.). Retrieved January 26, 2023, from https://www.drugs.com/rituximab.html
5) Salles, G., Barrett, M., Foà, R., Maurer, J., O’Brien, S., Valente, N., Wenger, M., & Maloney, D. G. (2017). Rituximab in B-cell hematologic malignancies: A review of 20 years of clinical experience. Advances in Therapy, 34(10), 2232–2273. https://doi.org/10.1007/s12325-017-0612-x
6) Weiner, G. J. (2010). Rituximab: Mechanism of action. Seminars in Hematology, 47(2), 115–123. https://doi.org/10.1053/j.seminhematol.2010.01.011
Leave a Reply